
ARTICLE Categories
All
|
If one-size-fits-all diets worked, don’t you think we would know the magic formula by now?1/24/2023 My 5 top tips to finding out what eating style works for you Hands up if you’ve seen or heard something about a magic formula that results in weight loss, more energy, miracle reduction in x, y, or z symptoms and all in record time. Maybe you saw something on the television, read it in a magazine or even witnessed a friend being transformed in front of your own eyes.
Now hands up if you tried it yourself. You bought the book/programme and lined yourself up to follow the same plan. If I might hazard a guess, it didn’t have quite the same miraculous effect. What do you think happened? Please don’t tell me that you blamed yourself. If you did, remember this: If one-size-fits-all diets worked, don’t you think we would know the magic formula by now? Finding out what works for you and your lifestyle is the key to it all and in this article, I will give you five ways to explore what that is.
Please note that these tips do not provide any nutritional advice. If you are looking for personalised recommendations to support a specific health issue, you should contact a nutrition or health professional. I offer free (no-obligation) introductory calls if you wish to explore this avenue further. You can book for an adult here or a child here. You know yourself much more than you think you do, so here are my 5 top tips to help you discover what works for you. 1. In your experience, in the past, what has worked, not worked, or worked but not been sustainable? Get a piece of paper and divide it into three columns. Think back to what has worked for you in the past. Was there a time in your life where you were eating a certain way or following certain habits and you felt amazing? Or how about things that you tried but realised didn’t suit you? Please don’t include those times where you crashed dieted to fit into a certain outfit for a certain event. Use the three columns to divide your recollections into things that worked, things that didn’t and finally things that you thought worked but were not sustainable long term. Remember that the things that worked or didn’t, could be a patchwork of things from different periods in your life. At university it may have been the sport, during your first job it could have been enjoying a loaded coffee and muffin every day on your way in and more recently it could be that you tried apple cider vinegar in water before a meal, but you hate the taste, and it gave you heartburn. Don’t just do this exercise in one go, keep coming back to it and adding to the recollections. Review what you have written. Which things in the ‘didn’t work’ column do you find yourself still doing now and that you probably could set to one side? Which in the ‘did work’ had you forgotten about and think that you could reincorporate into your daily life. Finally, are there any in the ‘worked but not sustainable’ column that you could adapt so that they do work for you long term? 2. Keep a record. I work with a lot of clients (adults and children) who suspect that there are foods that don’t suit them. One of the first things I do is ask them to keep a food and symptom diary so that we can, perhaps, identify patterns or triggers. I have a free tool for recording this available here. If you are trying to find out which ways of eating suit you, then you would also benefit from recording what you eat, but instead of writing down what symptoms occur, although you can include those too, you would write down how you felt after a meal. After a baked potato, did you feel great and were able to power through to the next meal without snacking or did you have an energy slump after about 30 minutes and want a nap? If you have breakfast, does that sustain you or does it open the door to feeling hungry for the rest of the morning? Can you identify any foods that bizarrely make you feel hungrier rather than satisfy you? What else have you spotted that give you clues? To find out how we should eat, we need to be an observer of how we feel. Consider it doing your own scientific study. Recording isn’t for everyone, however. If you find yourself spending a bit too much time recording things, then this tip isn’t for you, and you would do better letting it go. We can be too caught up in the detail, the idea is to see the bigger picture and relax about the whole. 3. Use your imagination, but be realistic Now that you’ve sifted through your recollections it’s time to use your imagination. If you could design a way of eating based on what you know about yourself, which fits with your values and is sustainable forever, what would it look like? This tip is about not only choosing foods that suit you in terms of nutrition, but also suit your lifestyle and budget. Whichever way of eating suits you best, be it omnivore, low carb, plant-based or other, must be practical. Otherwise, with all the will in the world, you won’t keep it up. Consistency is the key. Consistency in your eating habits, body movement and lifestyle choices. So, if you could design your perfect nutrition and lifestyle habits, what do you think they would be? Once you have that vision in your mind start implementing them. Don’t go too fast though! It’s easy to do all and then nothing. Introduce one thing at a time, when you feel as if it is integrated into your life, then move on to the next. 4. Don’t get hung up on the hype. This past month has seen the publication of multiple articles predicting this year’s superfoods. Don’t get me wrong, there are some foods that are absolute powerhouses of nutrition, but it doesn’t mean that that you will be under-nourished if you don’t have them. You could go out and spend a fortune on the new wonder food, but there is probably a more local, cost-effective food that will do just as well and that you could eat more regularly. A diet that suits you is one that suits every aspect of your life. 5. What to do if you DO want to follow a certain diet but your body rebels? Ethical, cultural, or religious reasons can make you want to eat a certain way, even if you can sense that it isn’t the best way to eat for you. My advice in these cases is to take it slow and steady. Research has shown that our gut microbiome adapts itself to our diets. Whatever you are eating on a regular basis is reflected in the bacterium types in your gut. Changing your diet suddenly can cause digestive issues simply because there aren’t the right gut bacteria to digest and process the new foods. I always tell my clients to slowly introduce the new way of eating at a pace that allows the new microbiota population to grow at a similar pace. At the right time you may reach a tipping point where you can eat the new diet with no problems. If you are having continued issues with adapting your diet, then it may be best to get the support of a nutrition or health practitioner. So, to summarise my tips:
Read more, here are some of my previous blogs that you may find helpful:
To easily keep up with my articles, masterclasses, ebooks and online programmes and receive exclusive access to early bird offers, sign-up to my newsletter. My current newsletter features an early bird offer for my brand new online, self-guided course ‘Unleash the Change. Discover the habits and barriers hampering your efforts’. Sign-up to my newsletter now to benefit. Interested in what I do and who I am? Go to my website: www.jessicafonteneaunutrition.com
0 Comments
 You know that your symptoms are triggered by something, but you are unsure what. What can you do to decipher those triggers, without removing everything out of your diet and risking your health?
Here’s a quick overview of the information you will find:
Allergies, intolerances, and sensitivities – what’s the difference? There are three categories of food reaction – allergies, intolerances, and sensitivities. Each category has its own severity level. This is a big topic on its own and will covered by itself in next week’s blog. Here’s a quick overview:
If you suspect a reaction to food, then the first thing to do is to flag it to your medical practitioner. Depending on your symptoms your doctor may refer you for allergy testing. Ruling out a potentially serious allergy is vital. Having a diagnosed IgE allergy makes things clearer. There is a medical reason for eliminating that food from your or your child’s diet. If all your allergy tests come back negative, however, but you know that certain foods trigger a reaction, then that is where the complications can set in and it’s time to start deciphering which foods might be the culprit. My first piece of advice remains to consult with a nutrition professional before eliminating one or more food groups. What are elimination diets and why they may not be the answer There is a whole raft of symptoms that can be linked to food triggers. The most common are linked to digestion or skin conditions,, but others can include anything from joint pain to brain fog. One of my clients complained of falling asleep within 10 minutes of eating one square of chocolate! Most of my consultations relate to bloating, acid reflux, stomach pain and skin flares including acne, psoriasis, and atopic dermatitis/eczema. Elimination diets can be as simple as removing one suspected food, to removing many foods for a short period of time, under practitioner supervision. Well-known elimination diets include gluten or dairy free and the FODMAP diet. A more in-depth article on the FODMAP diet is planned for later this year. It is important for me to get this point across. It can be dangerous to follow an elimination diet long-term, especially if it excludes several food groups. My clinical experience has taught me that there is often just one or two true intolerances and sensitivities, which can often start a cascade of inflammatory responses that result in other, innocuous foods, causing reactions. In other words, continuously eliminating more and more foods is not the answer. It often seems that the more a person removes, the more they react to. A vicious cycle without end. Why elimination diets can be dangerous for infants and children and what to do instead Unless there is a diagnosed allergy, eliminating a whole host of foods is dangerous for infants and children. Any removal of individual foods or food groups should only be undertaken with the support of nutrition practitioner, so that this can be achieved safely and with no long-term consequences. Drastic eliminations can not only result in malnutrition, but for the younger population it can turn an unpleasant but innocuous intolerance into a full-blown diagnosed allergy. Infants and children have ‘naïve’ guts. Their gut microbiome (the useful bacteria we all have) is unformed and their immune response underdeveloped. Once foods have been eliminated for some time from this environment, it can be very difficult for those foods to be reintroduced. Subsequent symptoms can be stronger and last longer, even without the development of an allergy. Working with infants and children my aim is always to cautiously remove a highly suspected food and only for a very limited amount of time. My ultimate objective is always to expand the child’s diet as much as possible to support the development and health of their gut microbiome. In my clinical experience, food triggers in children often resolve as their gut and immune systems grow more robust. You think you might have an intolerance or sensitivity, what now? I find that clients who consult with me usually fall within one of three main groups.
They all have the same thing in common, a need to move past the symptoms and start eating in a way that suits them. A Food and Symptom Diary, a great self-help tool It can often be difficult to unravel which foods cause which symptoms. Reactions from one food can transpose or hide reactions from another and not all foods trigger the same symptoms. Digestive symptoms often appear quickly after the problem food, however skin conditions, specifically atopic dermatitis/eczema can take up to 72 hours to manifest. Keeping a record of what you eat and drink and any symptoms that appear can help you uncover patterns that would otherwise have been missed, especially with delayed onset reactions. For example, you’ve had a bad eczema flare and when you look back at your food and symptom diary you can see that prior to each of the last few flares you’ve eaten such and such a food. It may not be the full story, but it’s a definite place to start. The thought of completing a daily food and symptom diary can be daunting for some. So, for those clients who don’t want to do it daily, I suggest that they log the previous 24-72 hours’ worth of food after the development of a symptom. There is a proviso, however, this recall can sometimes be problematic. Humans are notoriously selective in their memory’s. Details can be forgotten, especially after 72 hours. I have a free Food and Symptom Diary tool on my website that anyone can download for free. https://tinyurl.com/4rpwnwrd . How can you be sure if a symptom is linked to a food or not? When a person is being hypervigilant about monitoring their food and symptoms, they can sometimes naturally interpret some symptoms as related to certain foods when they, in fact aren’t. This can be because of a variety of reasons including delayed-onset symptoms, or because some foods are harder to digest regardless of whether you have a digestive condition or not. Research increasingly points to intestinal hyper-permeability (leaky gut) as a root cause of multiple food reactions or it could just be because the gut is so inflamed from a genuine, unidentified trigger, that it starts reacting to random other things. As a Registered Nutritional Therapist, I work with my clients to decipher the level of symptom it might be. Using a traffic light analogy, is it a red symptom that we should absolutely pay attention to or is it a more ambiguous amber? Removing lots of foods might seem to make sense, but it may not be right My suspicions are aroused when a client says that they can eat fewer and fewer foods. This usually indicates that a red symptom trigger is setting off a cascade of inflammation which then causes a raft of ambiguous amber symptoms. Then there is also the consideration, is it a false amber? Could it be manifesting because of the underlying red trigger? Or is it in fact a true amber? This would mean that it does cause symptoms but not to the same extent as a red trigger and it could, potentially, be eaten not too often and not too much. To sum up, my top tips
Read more: What is the atopic march? Why is eczema/atopic dermatitis itchier at night? You’ve been diagnosed with an atopic condition, but what does that mean? Atopic dermatitis/eczema – a chronic condition that effects all ages The skin microbiome, the key to good skin health Autumnal Allergies – Yes it is a thing To easily keep up with my articles, masterclasses, ebooks and online programmes and receive exclusive access to early bird offers, sign-up to my newsletter Interested in what I do and who I am? Go to my website: www.jessicafonteneaunutrition.com  It’s autumn, you begin to heave a sigh of relief thinking that the hay fever and seasonal allergies season is finally over. Then you realise that you are still getting symptoms – itchy eyes, runny nose, a dermatitis flare, and that you are suffering from autumnal allergies.
TV adverts and magazine articles would have you think that hay fever and seasonal allergies only happen in the spring and summer, but that isn’t the case. Autumn brings its own set of allergens ready to trigger a runny nose, atopic dermatitis, and itchy eyes. If it isn’t plant pollen, what are the autumnal triggers that can cause so many issues? Weed pollen, mould spores and house mites are the most common triggers for Autumnal allergies, read on to find out more details and to get my 5 tips to lessen the autumnal allergy symptoms. Weed Pollen Not all pollen producing plants flower in spring. A whole category of weeds flower in the autumn and produce the highly allergenic weed pollen. These plants usually flower from late August until the first frost (usually around the end of November but growing later with climate change). This category of plants includes common weeds found in the UK such as nettles and sorrel but also varieties that are much newer to the UK and Europe such as the American Ragweed. Not only is ragweed a recent invader, but it also produces one of the highest amounts of pollen, causing uncomfortable hay fever and dermatitis symptoms in many sufferers. Mould Spores Mould is around us all the time, but at this time of year levels peak with the falling leaves gently composting on the ground releasing large amounts of allergenic spores. These are the main types of mould which have been highlighted as being triggers for allergy symptoms:
Dust Mites Many sufferers of asthma, eczema or hay fever also have a dust mite allergy and whilst dust mites exist all year, reactions tend to peak in autumn as the weather becomes damp but remains relatively warm and we retreat inside and close our doors and windows, but we haven’t yet put our heating on. 5 Tips to Lesson the Autumnal Allergy Symptoms
If you were interested in this article, you may be interested in these other blogs I’ve previously published: What is the atopic march? Why is eczema/atopic dermatitis itchier at night? You’ve been diagnosed with an atopic condition, but what does that mean? Atopic dermatitis/eczema – a chronic condition that effects all ages The skin microbiome, the key to good skin health To easily keep up with my articles, masterclasses, ebooks and online programmes and receive exclusive access to early bird offers, sign-up to my newsletter Interested in what I do and who I am? Go to my website: www.jessicafonteneaunutrition.com  We’ve all heard about the gut microbiome (population of bacteria) but did you know that your skin had its own microbiome? We now know that that skin microbiome is implicated in several skin health conditions including Atopic Dermatitis (AD) but also acne, rosacea, and psoriasis. Research has shown that the skin and intestinal microbiomes are similar in a number of ways:
Treatment usually focuses on antimicrobial and antibiotic creams and current research is looking into crems that target the over abundant staphylococcus strains specifically. How to support your skin microbiome Your skin and gut microbiomes are closely linked, so here are my top tips for maintaining a healthy skin microbiome:
References 1. Szari S, Quinn JA. Supporting a Healthy Microbiome for the Primary Prevention of Eczema. Clin Rev Allergy Immunol. 2019;57(2):286–93. 2. Martinez KB, Leone V, Chang EB. Western diets, gut dysbiosis, and metabolic diseases: Are they linked? Gut Microbes [Internet]. 2017;8(2):130–42. Available from: http://dx.doi.org/10.1080/19490976.2016.1270811 3. Nakatsuji T, Gallo RL. The role of the skin microbiome in atopic dermatitis. Ann Allergy, Asthma Immunol [Internet]. 2019;122(3):263–9. Available from: https://doi.org/10.1016/j.anai.2018.12.003  The Atopic March is the term given to the progression of allergic or atopic conditions from infancy into childhood. The ‘march’ usually starts with atopic dermatitis/eczema (AD in babies and sometimes progresses to food allergy, asthma, and allergic rhinitis (hay fever), Don’t panic! Just because there is an atopic march, it doesn’t mean that every infant or child who has AD will go on to develop any of the atopic conditions listed ! Only 60% of children with severe AD go on to experience other conditions within the Atopic March and for those with mild AD, the figure is only 20%. 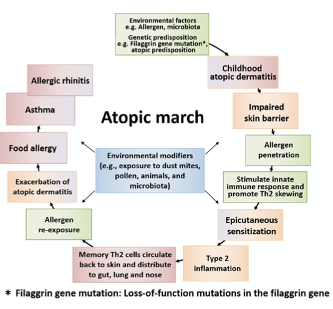 Figure taken from Tsuge et al., (2021) (1) highlighting the atopic march and some of the different factors thought to be involved. The reasons behind the Atopic March as like those thought to be behind AD generally. A fragile skin barrier that lets possible food or environmental allergens in, triggering the activation of an immune response. Once the initial reaction has been experienced, the body identifies the food or environmental particle as an ‘enemy’ and reactions will manifest either as continuing AD or via other reactions such as hay fever, food allergy or even asthma. (2)
Nutritional strategies for infants and children who may have a familial susceptibility to atopy:
References 1. Tsuge M, Ikeda M, Matsumoto N, Yorifuji T, Tsukahara H. Current insights into atopic march. Children. 2021;8(11):1–17. 2. Yang L, Fu J, Zhou Y. Research Progress in Atopic March. Front Immunol. 2020;11(August):1–11. 3. Davidson WF, Leung DYM, Beck LA, Cecilia M, Boguniewicz M, Busse WW, et al. J Allergy Clin Immunol. 2020;143(3):894–913.  No, it isn’t your imagination that your, or your child’s, eczema is itchier at night. Keep reading to find out more and to get some tips on how to alleviate this occurrence:
Cortisol, the body's natural anti-inflammatory. Levels of our hormones go up and down throughout the day for a variety of reasons, depending on their purpose. One of our main hormones, cortisol is high in the early morning to help wake us up and then lowers as the day progresses until it reaches its lowest level at bedtime, allowing us to become sleepy and have a good night’s rest. Cortisol also has anti-inflammatory effects, which helps naturally dampen eczema’s itchiness and flare. When cortisol levels are naturally low, inflammation will rise, and eczema’s affects will be more readily felt. Hence the night-time itch. The aim for all eczema support is lowering inflammation, often with medication such as hydrocortisone. However, identifying triggers for eczema flares whether environmental, stress or nutrition is ideal for keeping eczema flares and inflammation down. However, they can be tricky to pinpoint, and you should get support from a health or nutrition professional. Some foods are known for their anti-inflammatory properties such as oily fish (sardines, mackerel, salmon), nuts and seeds and green leafy vegetables. Other foods such as ultra-processed foods and drinks can have a more inflammatory effect on the body and so it may be wise to limit those, especially in the evening. Keep cool. For many, temperature differences can be a flare trigger. Too cold and the skin dries and becomes chapped and too hot and the blood vessels nearest the skin barrier, expand, triggering inflammatory cells, raising inflammation, and causing an itch. Consider introducing lighter bed clothes or a weighted blanket with a lower tog if you prefer the feeling of being tucked in. Putting towels in the freezer and then applying them to the itchier parts of the body can be soothing. Natural versus man-made material sheets. Man-made sheets including polyester or nylon are less breathable and can result in more sweating which releases natural body salts which can irritate the skin. Consider investing in cotton or linen sheets which are more soothing to the skin. The only exception to that rule is a wool blanket, the natural lanolin it contains can be extremely triggering for eczema and should, therefore, be replaced with a thin fleece blanket or tucked-in, in a way that so that none of the wool touches the skin. Keep dust at bay. Most eczema sufferers have issues with dust mites and simply dusting the bedroom daily and regularly hoovering under the bed may already lessen a nocturnal flare. Rehydrate. We tend to lose a lot of moisture during the night and so we need to think of hydration both from the inside, by ensuring that we drink plenty of water during the day, but also the outside by moisturising before bedtime to help maintain the skin barrier. If you want to know more about what I do and how I can help, please visit my website: www.jessicafonteneaunutrition.com  If you or a loved one has been diagnosed with ‘atopic’ eczema or dermatitis you might be wondering what the ‘atopic’ bit means.
Basically, atopy is the term used to describe those people who develop allergic conditions including allergic rhinitis (including hay fever), asthma and atopic dermatitis/eczema (AD). It usually means that the diagnosed individual has greater immune response, or ‘atopic reaction’ to common allergens including environmental triggers such as pollen and grasses etc.) and food. Atopy versus Allergy Atopy is a Type I hypersensitivity reaction, which means that there is an immediate hypersensitivity to an antigen which results in an over-exaggerated IgE mediated immune response. Allergies are an exaggerated immune response regarding of the mechanism. This means that whilst all atopic reactions are considered allergies, not allergies are considered atopic. Could Irritable Bowel Syndrome (IBS) be atopic? In 2008 scientists published a paper naming a new subtype of IBS, atopic IBS (1). More recent studies appear to confirm the connection between atopy and IBS, with those diagnosed with atopy being at much higher risk for IBS and even Intestinal Bowel Disease. (2,3) Which symptoms are linked to atopy?
Nutrition and atopy Nutrition to support an atopic medical diagnosis will need to be individualised to the food or environmental triggers involved and the specific atopy – skin, gut, lung etc. If you would like to hear more about how nutrition could support your atopy diagnosis, please book in to tell me your story. https://p.bttr.to/2Lh2ifV References 1. Tobin MC, Moparty B, Farhadi A, DeMeo MT, Bansal PJ, Keshavarzian A. Atopic irritable bowel syndrome: a novel subgroup of irritable bowel syndrome with allergic manifestations. Ann allergy, asthma Immunol Off Publ Am Coll Allergy, Asthma, Immunol. 2008 Jan;100(1):49–53. 2. Walker MM, Talley NJ, Keely S. Follow up on atopy and the gastrointestinal tract – a review of a common association 2018. Expert Rev Gastroenterol Hepatol [Internet]. 2019 May 4;13(5):437–45. Available from: https://doi.org/10.1080/17474124.2019.1596025 3. Koloski N, Jones M, Walker MM, Veysey M, Zala A, Keely S, et al. Population based study: atopy and autoimmune diseases are associated with functional dyspepsia and irritable bowel syndrome, independent of psychological distress. Aliment Pharmacol Ther. 2019 Mar;49(5):546–55.  Atopic eczema or dermatitis (AD) often starts in infancy and the good news is that for most children it spontaneously resolves by the age of seven. However, AD doesn’t like to conform and so for some, AD remains until puberty, may return in later adulthood and for the very unlucky stays with them throughout their lives. Unfortunately for some children, the early onset of AD also signals the start of the ‘atopic march’, with the appearance of hay fever and even asthma, either in tandem with the AD or in some cases instead of (1). In addition, whilst more boys are diagnosed with allergies in childhood, in adulthood women are significantly more likely to be diagnosed with a food allergy and the menopause has been identified as a time when AD flares can either increase or disappear. (17,18). So why do some people get AD? Helping clients with AD is my vocation, as I have suffered from this condition since I was 6 months old. I am so interested in this topic that I have just completed a Master of Science with a dissertation entitled: ‘Examine how nutrition can be used as a complementary tool for the support of eczema/chronic atopic dermatitis (AD)' and I will share some of what I learnt below: Multiple causes have been identified including skin barrier disruption, mutations in the filaggrin gene, gut microbiome (gut bacteria) imbalance, as well as immunological (allergy/intolerances) and environmental triggers, yet there is still no definition of what causes AD. This lack of definitive cause leads to dermatologists and allergy specialists telling their patients that eczema is uncurable and that it can only be modulated by use of corticosteroids and other topical creams and emollients (2,3). There are, however, several areas of research that might shed more light. You may have heard of leaky gut, but it could be that AD sufferers have leaky skin which may be caused by the mutation of a skin protein gene called filaggrin (FLG). Basically, FLG is used to seal the skin barrier and acts to both stop water loss and potential pathogens crossing into the bloodstream. What this means in practice is that whilst the water loss creates the dry, flaky and itchy skin so well-known to eczema sufferers, the ‘leaky skin’ could also be allowing environmental and even food allergens to cross, triggering an immune reaction and inflammation. Up to 48% of AD sufferers have been found to carry this mutated FLG gene (FLG-null-allele) which makes it a very exciting area of research. (4–6). The FLG research has also been linked to another area of AD research, the ‘dual allergen exposure hypotheses’ (12) relating to inappropriate immune response. This area of research suggests that the FLG affected ‘leaky skin’ exposes the AD sufferer to food antigens via touch. The food particle enters the bloodstream via the skin and is quickly identified as a foreigner by the person’s immune system. This causes the body to go into high alert, triggering inflammation and labelling that food antigen as a future threat. A vicious cycle then ensues with the inflammation causing further damage to the skin barrier and leading to even more risk of exposure to food and environmental antigens. Recent studies have found that this type of food antigen exposure can lead to subsequent ingested food sensitivities and intolerances and provides a potential explanation as to why so many AD sufferers know that they react to certain foods, despite negative allergy testing. (13). Studies have shown that child AD sufferers are at higher risk of IgE mediated food allergies but also non-IgE Mediated (delayed) allergies (14). Diagnoses are made via either a blood draw to test for specific IgE antibodies or via Skin Prick Test (15). Other possible tests include the Atopy Patch Test, IgG testing and the Elimination Diet. In children caution must be applied to the Elimination Diet as it is thought that continuous consumption of a trigger food will result in it being better tolerated and that the removal of this food from the diet for a period may result in an increased risk of severe allergy or even anaphylaxis (16). The gut microbiome has become a key research focus within the last decade, both in terms of health generally but also specifically in relation to AD. Intestinal hyperpermeability (leaky gut) and gut microbiome (bacteria) imbalance are linked to worsened immunity, higher rates of inflammation and risk of allergies and intolerances. AD patients have been identified as being at higher risk of both these (10,11). Recently research has started to focus on the skin microbiome (bacterial population). This research has identified that individuals with atopic eczema suffer from skin microbiome dysbiosis (imbalance) with a skew to an overgrown population of staphylococcus epidermidis and staphylococcus aureus (7,8). My clinical experience has often found individual clients who demonstrate a link between both skin and gut dysbiosis (9) and this is an area I am passionate about. Nutritional Strategies As mentioned in the introduction, AD doesn’t like to conform. Whilst there are some common recommendations to all AD sufferers, no two nutrition recommendations are alike, just like no two people’s skin or gut microbiomes are alike. What may work for one, will not work for another. Supporting clients with this condition involves the combining of many pieces of information with practitioner knowledge. Seeking out the individualised manner of eating that allows that person to eat the most varied diet possible, whilst being aware of those foods and environmental triggers that may cause a flare. The main objective is to provide the empowerment that allows for each client to have a sense of control, whilst having the knowledge to face new challenges, in line with AD’s non-conformist tendencies. Below are some of the key nutrients that research has found to be supportive for AD sufferers:
Whilst a deficiency in zinc status has been long thought to be linked to AD, studies using supplementation did not show any benefits (25,26). References:
1. Ring J, Zink A, Arents BWM, Seitz IA, Mensing U, Schielein MC, et al. Atopic eczema: burden of disease and individual suffering – results from a large EU study in adults. J Eur Acad Dermatology Venereol. 2019;33(7):1331–40. 2. Nutten S. Atopic dermatitis: Global epidemiology and risk factors. Ann Nutr Metab. 2015;66:8–16. 3. Lopez Carrera YI, Al Hammadi A, Huang YH, Llamado LJ, Mahgoub E, Tallman AM. Epidemiology, Diagnosis, and Treatment of Atopic Dermatitis in the Developing Countries of Asia, Africa, Latin America, and the Middle East: A Review. Dermatol Ther (Heidelb) [Internet]. 2019;9(4):685–705. Available from: https://doi.org/10.1007/s13555-019-00332-3 4. O’Regan GM, Sandilands A, McLean WHI, Irvine AD. Filaggrin in atopic dermatitis. J Allergy Clin Immunol. 2008;122(4):689–93. 5. Barbarot S, Aubert H. Physiopathologie de la dermatite atopique. Ann Dermatol Venereol. 2017;144:S14–20. 6. Bergqvist C, Ezzedine K. Vitamin D and the skin: what should a dermatologist know? G Ital di dermatologia e Venereol organo Uff Soc Ital di dermatologia e Sifilogr. 2019 Dec;154(6):669–80. 7. Szari S, Quinn JA. Supporting a Healthy Microbiome for the Primary Prevention of Eczema. Clin Rev Allergy Immunol. 2019;57(2):286–93. 8. Martinez KB, Leone V, Chang EB. Western diets, gut dysbiosis, and metabolic diseases: Are they linked? Gut Microbes [Internet]. 2017;8(2):130–42. Available from: http://dx.doi.org/10.1080/19490976.2016.1270811 9. Nakatsuji T, Gallo RL. The role of the skin microbiome in atopic dermatitis. Ann Allergy, Asthma Immunol [Internet]. 2019;122(3):263–9. Available from: https://doi.org/10.1016/j.anai.2018.12.003 10. Szari S, Quinn JA. Supporting a Healthy Microbiome for the Primary Prevention of Eczema. Clin Rev Allergy Immunol. 2019 Oct;57(2):286–93. 11. Rinninella E, Raoul P, Cintoni M, Franceschi F, Miggiano GAD, Gasbarrini A, et al. What is the healthy gut microbiota composition? A changing ecosystem across age, environment, diet, and diseases. Microorganisms. 2019;7(1). 12. Lack G. Epidemiologic risks for food allergy. J Allergy Clin Immunol. 2008;121(6):1331–6. 13. Tricon S, Willers S, Smit HA, Burney PG, Devereux G, Frew AJ, et al. Nutrition and allergic disease. Vol. 6, Clinical and Experimental Allergy Reviews. 2006. p. 117–88. 14. Abuabara K, Margolis DJ. Do children really outgrow their eczema, or is there more than one eczema? J Allergy Clin Immunol. 2013;132(5):1139–40. 15. Dhar S, Srinivas SM. Food allergy in atopic dermatitis. In: Indian Journal of Dermatology. 2016. 16. Finch J, Munhutu MN, Whitaker-Worth DL. Atopic dermatitis and nutrition. Clin Dermatol [Internet]. 2010;28(6):605–14. Available from: http://dx.doi.org/10.1016/j.clindermatol.2010.03.032 17. Chen W, Mempel M, Schober W, Behrendt H, Ring J. Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy Eur J Allergy Clin Immunol. 2008;63(11):1418–27. 18. Pali-Schöll I, Jensen-Jarolim E. Gender aspects in food allergy. Curr Opin Allergy Clin Immunol [Internet]. 2019;19(3). Available from: https://journals.lww.com/co-allergy/Fulltext/2019/06000/Gender_aspects_in_food_allergy.12.aspx 19. Rusu E, Enache G, Cursaru R, Alexescu A, Radu R, Onila O, et al. Prebiotics and probiotics in atopic dermatitis. Exp Ther Med. 2019 Aug;18(2):926–31. 20. Kim MJ, Kim SN, Lee YW, Choe YB, Ahn KJ. Vitamin D status and efficacy of vitamin D supplementation in atopic dermatitis: A systematic review and meta-analysis. Nutrients. 2016;8(12):8–17. 21. Navarro-Triviño FJ, Arias-Santiago S, Gilaberte-Calzada Y. Vitamin D and the Skin: A Review for Dermatologists. Actas Dermosifiliogr. 2019 May;110(4):262–72. 22. Balić A, Vlašić D, Žužul K, Marinović B, Bukvić Mokos Z. Omega-3 Versus Omega-6 Polyunsaturated Fatty Acids in the Prevention and Treatment of Inflammatory Skin Diseases. Int J Mol Sci. 2020 Jan;21(3). 23. Williams HC, Chalmers J. Prevention of Atopic Dermatitis. Acta Derm Venereol. 2020 Jun;100(12):adv00166. 24. Thomsen BJ, Chow EY, Sapijaszko MJ. The Potential Uses of Omega-3 Fatty Acids in Dermatology: A Review. J Cutan Med Surg. 2020;24(5):481–94. 25. Gray NA, Dhana A, Stein DJ, Khumalo NP. Zinc and atopic dermatitis: a systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 2019 Jun;33(6):1042–50. 26. Vaughn AR, Foolad N, Maarouf M, Tran KA, Shi VY. Micronutrients in Atopic Dermatitis: A Systematic Review. J Altern Complement Med. 2019 Jun;25(6):567–77.  More and more of us are interested in modifying our diet to better support our planet, but many of us are lost with how to support our aims without compromising our nutrition.
This is an area for which I have a particular interest. In February 2019 I published an article entitled Nutrition Recommendations in the Age of Climate Change within my professional association (bant.org.uk) newsletter. With more and more clients coming to see me to ask for help in this area I thought that it would be best to undertake some further training and to check whether my knowledge was still up to date to be able to support my clients best. Last week I attended the Sustainable Food Choices Nurturing Human Health and the Planet course run by @christinebailey for @ION which also featured the supremely knowledgeable @realfoodcampaign. Combining this knowledge from both my own research and last week’s course here are my top tips !
 Does this sound familiar?
One of the solutions proposed to help support the planet is to introduce more plant-based meals to our diet, and with vegan and vegetarian options becoming more easily available many of us are embracing this new way of eating with gusto. The trouble is, changing your diet radically and in a short period of time can result in a host of digestive issues, including bloating, indigestion, flatulence, and pain. It is important to note here that any persistent digestive issues should be checked by your GP, but if you can link the digestive symptoms to your new diet then the answer may simply be that your gut and the good bacteria (microbiome) it houses isn’t primed to digest those foods. We all have a variety of different bacteria in our gut and different bacteria like eating different things. If you’ve been traditionally a ‘meat and two veg’ type of eater, then your microbiome population will be geared towards those foods. If you have traditionally rarely eaten legumes and your fibre intake was low, the bacteria population that likes those things may be small and struggle with the sudden influx. There simply isn’t enough of those bacteria to process the new diet. The secret is to gradually increase your plant-based foods rather than suddenly go all in. As you increase your intake of fibre and legumes such as chickpeas, lentils, beans and peas, the population of bacteria that loves those foods will grow and so you will be able to tolerate more. Unfortunately, one of the main signs that this population is expanding is flatulence, but if you go gradually, it should be a temporary and should subside as as your gut gets accustomed to its new diet. |
AuthorI’m Jessica Fonteneau, I’m the eczema specialist and I help people Escape from the Eczema trap. Archives
April 2024
Catégories
All
|
 RSS Feed
RSS Feed